





Pathological studies
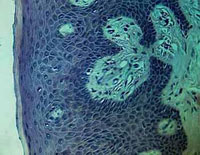
Cytological smears from the mouth-wash fluid mainly contained superficial, mature cells. In 17 smears of 3 patients with glass abutment amongst the 67 cytological specimen of 9 patients were found a few keratinized but otherwise typical cell beside the large number of non keratinized epithelial elements (figure 1/a.)
-

- obr. 1/a
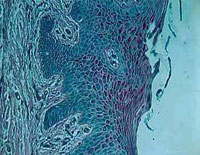
These three patients had bridges supported by two glass abutment built in 2-4 years before. There was no significant keratinization either in the specimens of the other patients with glass abutment supported bridges or in the precipitated mouth-wash fluid of control patients with traditional bridges. Typical keratinized stratified epithelium was present on the surface of the gum under the glass abutment (figures 2/a and 2/b). Keratinization corresponded to parakeratosis and hyperkeratosis histologicaly. There were no mitotic figures amongst the epithelial cells, layers of the epithelium presented typical maturation tendency towards the surface (figure 2/a.).
-

- obr. 2/a
-
- obr. 2/b
The applied fixative poorly fixed tissue glycogen, however the cytoplasm of the cells contained abundant glycogen (figures 3/a and 3/b)
-
- obr. 3/a
-
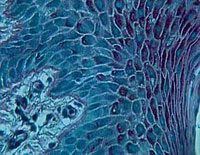
- obr. 3/b
In the control sections of the gingiva under the removable prosthesis as well as without the substitution of the teeth, the tendency of the keratinisation appeared even then the keratinisation layer appeared to be thinner than under glass abutment. (pic.4).
-

- obr. 4
With scanning electron microscopy the surface of the new abutment at the gingival side was smooth. Scraping, mechanical injury and deformity as subject of mucosal irritation were not found. Element composition measured at five different sites (within 350 micron in diameter areas) was practically the same. The surface and the chemical composition of the glass abutments implanted as long as eight months and one year equaled that of the new abutments. According to the cytological and histological studies it can be established, that the mucosa under the glass abutment showed mild but typical keratinous tendency, that was characterized as hyperkeratosis and parakeratosis and not as dysplasia of the precarcinomatous leukoplakia. Similarly to the mucosa of those with traditional bridges, removable prosthetics as controls and of those who chew on the gum, histologicaly there was a harmless, adaptive keratinization. The degree of keratinization was far below that of the leukoplakia noticed due to hot and spicy foods, meantime the cells remained typical. As a conclusion it can be stated, that cytological and histological changes of the mucosa under the glass abutment are not different in quality (only in quantity) from those noticed under traditional bridges, prosthetics and also from those patients who are without dentures and chew on their gum. DNA analysis was performed on Feulgen-Schiff specimen with the help of computer assisted histological image analysis program (DNASK). This program is able to determine 13 morpho- and densitometric parameters of the nucleus. The image analysis for DNA measurement within the basal cells of the epithelium of the three studied groups (with glass abutments, with removable
DNA analysis is useful in case of such procedure as morphologicaly completely similar tissue lesions can represent different prognosis if the cellular DNA content changes determined by naked eye or by microscopic examination. These changes can be the result of overloading when the DNA content simply doubles and polyploid, tetraploid cells develop, but when the epithelium displays inclination for dysplatic metaplastic change, that is precancerous stage, the DNA content not only doubles but irregularly changes, thus can be two and a half times or three times, three and a half times more than the normal. The result of DNA analysis indicated normal diploid tissue appearance in addition to a significantly lower tetraploid cell population, which could be due to mechanical stress, on the other hand we did not find aneuploid polyploidity that characterized precancerous stage (figure 5.). Summarizing the results of pathological studies, instead of the expected metaplastic, dysplastic changes that were reasonable from our general pathological knowledge, we found simple adaptive hyperkeratosis under the glass abutment, the degree of which did not even reach the degree of hyperkeratosis in patients who chewed on their gum. Glass abutment did not mean such mucosal stress that was caused by the direct gum chewing on the mucosa.

obr. 5 – Ploidy histogram
Static analysis
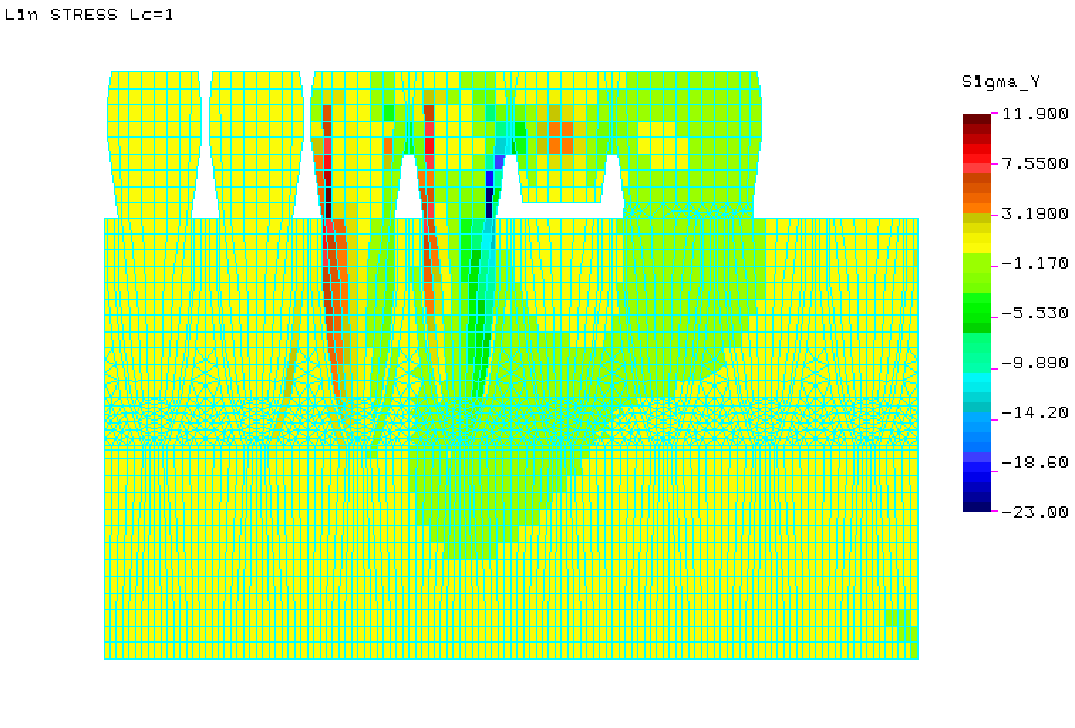
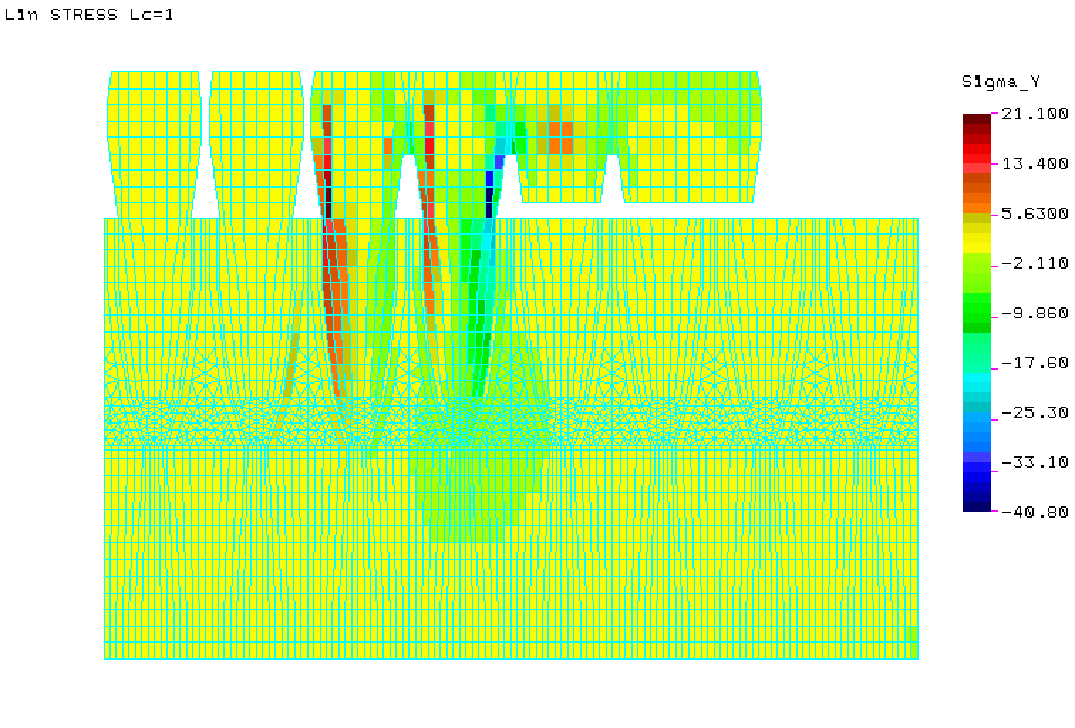
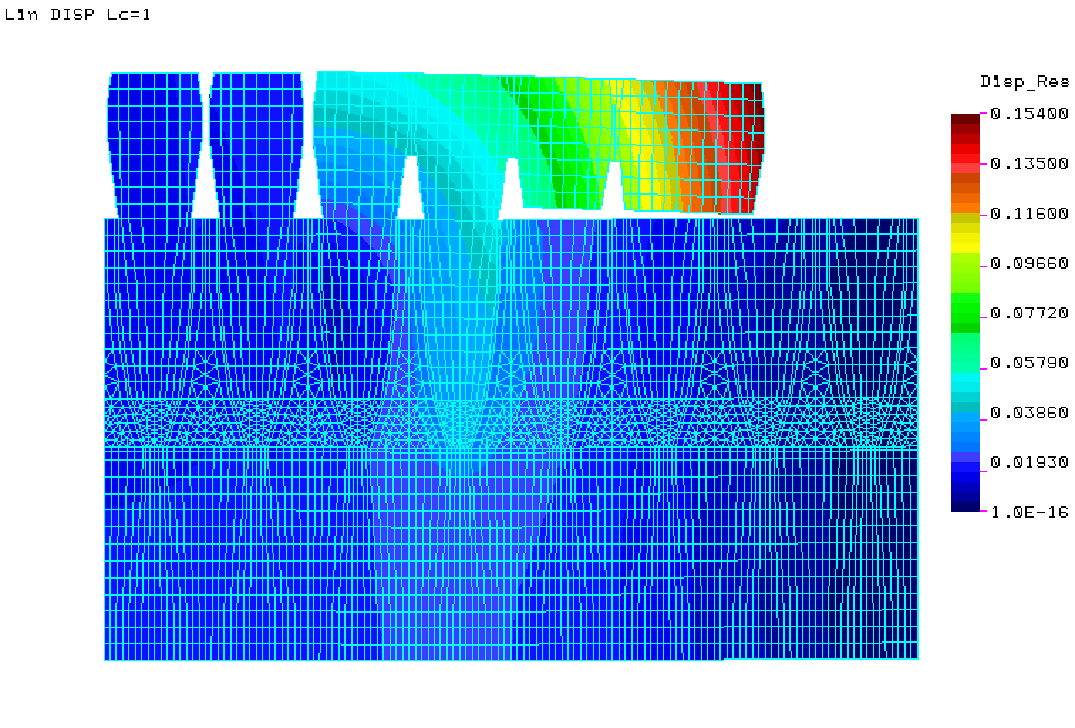
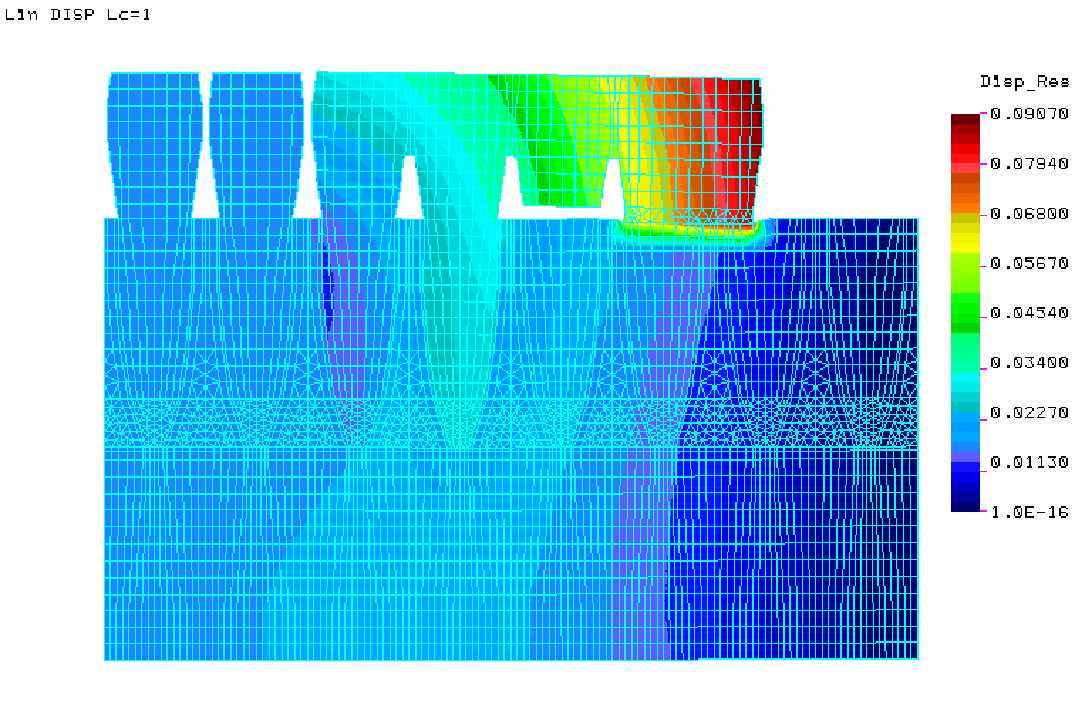
For the substitution of so called free end situations, employment of removable or anchored or supported bridge works are recommended according to the therapeutic indications accepted by the methodological letters. Utilization of removable denture is often rendered because of the patients’ aversion from such type of prosthetics or because of the biological or financial causes or the patients’ fear from the surgical intervention in case of implantation. The aim of our static analysis was to verify the importance and role of glass abutment in supporting and its function in conducting the consequent forces. Furthermore we wished to contradict the presume that ZX-27 did not at all differ statically or functionally from the practice of free end bridges. The Transient Element method served as tool of the study is suitable for answering the aimed, conceived and expected questions. It is obvious at first glance from the figures that the greatest importance of the glass abutment in force conduction and driving on supporting teeth is its relief role. Figure 6. well demonstrates that conduction of the consequent force much better acts on the two supporting teeth due to the glass abutment than in case of free end bridges (Figures 6-7.) The results of static analysis performed with Transient Element Method demonstrate that the prosthetic with glass abutment support does not work by the practical and theoretical system of the free end bridges.
-
- obr. 6
-
- obr. 7
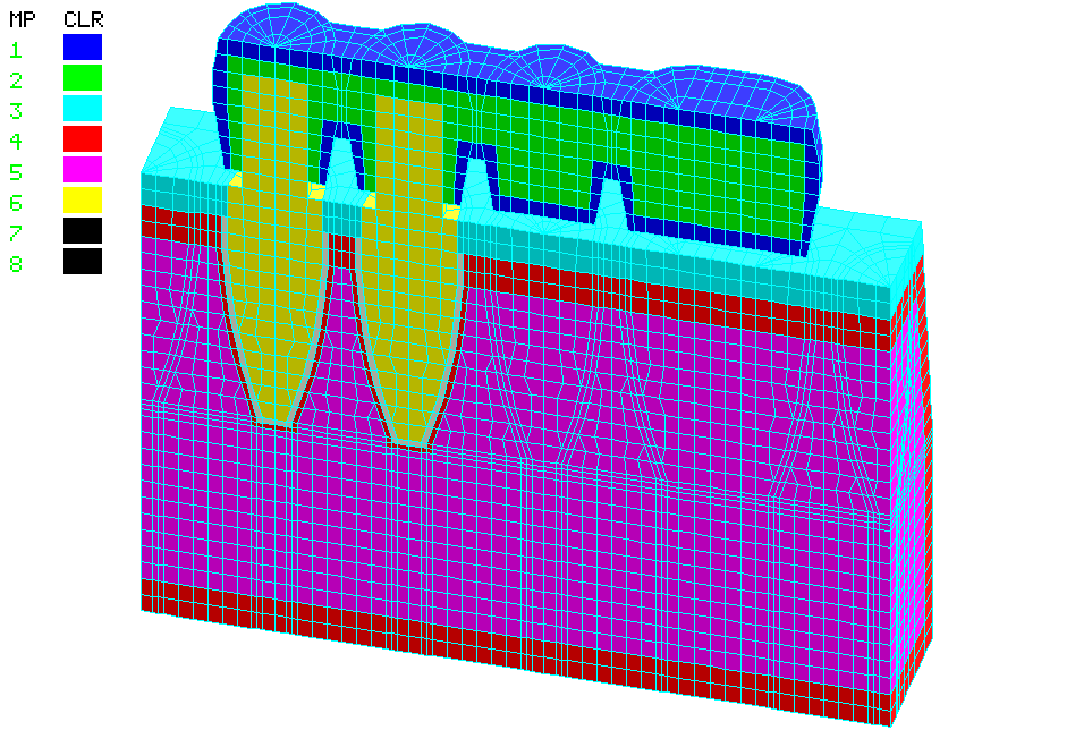
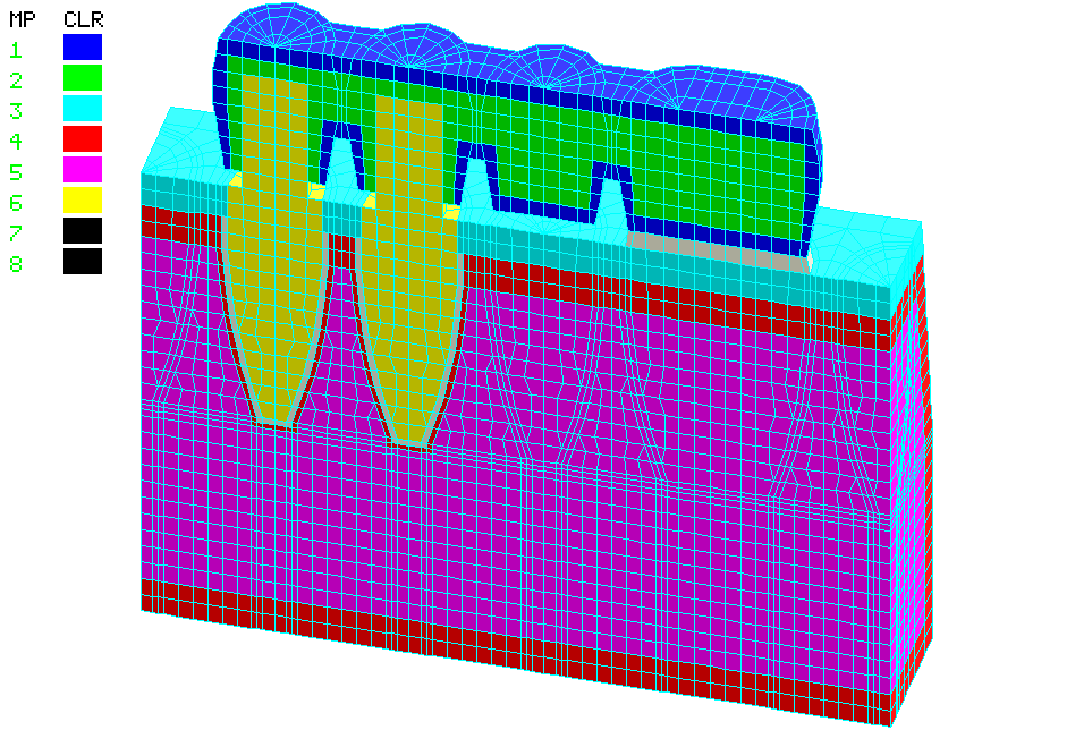
Although the data of technical literature were determined by the given data published in most recent worldwide journals and by our measured data, the accuracy of the measures were aggravated by the capacity of the applied PC-s or by the simplifications due to the presumably low effect of certain geometric characteristics. The following results developed: – gingiva is 2 mm in diameter – cortical bone is 3-3 mm in diameter – paradontium along the roote is 0,25 mm in diameter – thickness of cortical bone is 0.5 mm in diameter Indication of the remaining data was easier owning to the relatively more simply and accurate measurability of substance specificity. Such specificity are of the metals and ceramics employed during preparation of bridges that are summed in a table expressible by plastic modules and by a so called Poisson number. Because of missing data in the technical literature and as the continually changing, individually derived, personal characteristics are lacking, measurements may contain inaccuracy, but these results are below the presumed values of real data. It means that oral glass abutment would present better results if we could measure or model them. It so happens that in case of vertical and lateral forces support of concave surfaced glass abutment is more favourable in reality (this is characterized by lower equivalent potential), in contrast to the model calculation of the present plain glass surface (Figures 8-9). Concave surface can transmit a lower proportion of lateral force to the convex gum surface, thus decreasing the lateral bending force of the crown (Figures 10-11).
Consequently this study e.g. could not model the effect of pulsating forces on paradental fibers, mucosa-bone bad e.t.c. These effects were supported by further, mainly clinical, longitudinal experiments, that would be the point later. Evaluation of the results were rendered difficult as we could not obtain the documents of such measurements in relation to individual dentures. Here I principally think of the effect of consequent forces on the paradentium of existing teeth and of the measured results in case of model casted metal plates, partial uni- or bilateral anchoring. As after the pathological and static examinations, that previously questioned applicability of ZX-27 Attractive Glass Abutment System, had administered reassuring results and chronic toxicity, cytotoxic, genotoxic and biopersistency studies had presented negative results, it became necessary to examine what changes did the long lasting equipment cause on bone bad in contact to the surface.
-
- obr. 8
-
- obr. 9
-
- obr. 10
-
- obr. 11
Radiology
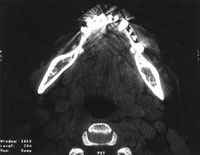
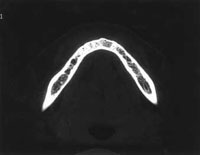
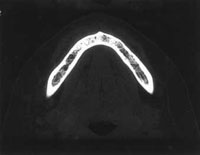
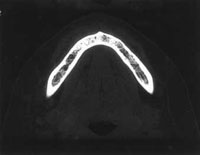
In case of accurate determination of the bone’s condition we did not principally use OP pictures employed in dentistry, but we elected to series of CT scan that can measure bone density. Traditional radiological method for examining dental alveolus is the thick layer shot, the so called panorama X-ray. It is extremely useful in designing the denture. It is also employed in examination of localized inflammatory bone resorption. However it is less applicable in quality estimation of the bones’ calcium content and completely inadequate for quantitative determination. That is why we performed computerized layer analysis within as thin layers as possible. With this method we can visualize the bone substance: the outer compact bone substance and the spongy substance beside (Figures 12-13).
-
- obr. 12
-

- obr.13
Densitometry can give indirect information on the calcium content. The question was further rendered difficult as every people had different skeleton that could be altered by the age, sex and way of living. Medical science has not been engaged in alveolar manifestations of osteoporosis. Therefore we can not give absolute results but we measured densitometric values of the surrounding and glass abutment carrying bone. Calcified trabecule and fatty marrow are always present within the measured volume. The former increase, the latter decreases density. The higher density value we measure, the higher is the calcium content. Measurements in the studied patients were performed between 27.06.1996. and 19.10.1999. Axial plain examination of the glass abutment carrying dental bed was performed natively within 1.5 mm in diameter slice thickness, from the body of the bridge works along the nearly complete volume of the bone structure. In pocession of the measured and calculated data we can tell that ZX-27 does not influence unfavourably the calcium content of the force bearing bone structure despite of its permanent contact with the gingiva, focal calcium loss (bone resorption) does not occur. Just the opposite! Measured values represent local strengthening of the bone (Figures 14-15).
-
- obr. 14
-
- obr. 15
Description:
Glass abutment system can be seen as hyperdensity structure on both sides (Figure 12.) beside the lower jaw. Arrows on the picture (Figure 13.) indicate thebone under the glass abutment system. The next two figures (Figures 14-15) demonstrate the bone structure at time of the first investigation. Thickness of external and internal layers of the bone correspond to that of the adjacent areas. The spongy structure has increased hyperdensity beneath the glass abutment system than of the neighbourhood, that means a higher mineral matter content. The next figures (Figures 16-19) show the bone structure at time of the second investigation. There is no change in thickness of both external and internal layers, spongy structure has an increased density compared to the neighbouring areas (A – arc in sqmm, M – density in Hounsfield units).
Conclusion:
During this 3 years period no resorption occured in the bone structure under the glass abutment system.
-
- obr. 16.
-

- obr. 17
-

- obr. 18
-

- obr. 19